
INNOVATIVE R&D
1. Intrinsic regenerative potential of human body clinically validated by MEBO
It is a long-held belief that the b ody has a full capacity to regenerate at the early gestation stage of the fetus, much less so during late gestation stages and early childhood; and an adult human body substantially loses its ability to regenerate. Instead, it goes down the default pathway of fibrotic repair which results in scarring and loss of physiological structure and function. Gurtner et al. (2008) “Wound repair and regeneration” Nature 453:314-321. Gurtner et al. (2007) “Progress and potential for regenerative medicine” Annu. Rev. Med. 58:299-312.
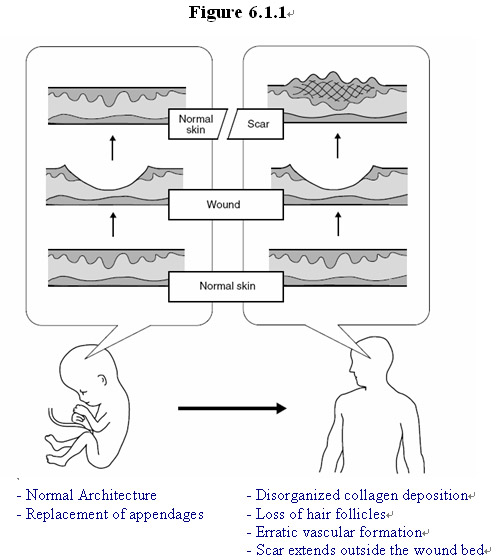
Take the body’s response to wound injury for example. According this prevalent belief in the field during the first two trimesters, the human fetus responds to injury by complete regeneration of the skin without scar formation. However, as intrauterine development progresses, this ability is lost. As shown in Figure 6.1.1, early fetal healing is characterized by complete regeneration of all cell types and correct architecture, whereas, with age, this regenerative capacity is lost and adult skin heals through scar formation.
As demonstrated in the clinical practice in the treatment of millions of wound patients, by using MEBO technologies and products, the injured skin and underlying tissue of adult humans can be regenerated with minimum scar formation and substantial restoration of physiological structure and function of the organ, including replaced skin appendages, orderly collagen fiber configuration, physiological networks of vascular and nerve. Lost fingers/toes of adult patients can be regenerated with near complete restoration of structure and function, including bones, muscles, nerves, blood vessels, connective tissues, fingernails and skin. As shown in Part VII of this book, recent preclinical and clinical data obtained by MEBO shows that internal organs of higher mammals and adult humans can be regenerated by oral delivery of MEBO products.
There results indicate that brought out by using the innovative technology and products provided by MEBO, the hidden regenerative potential of the body is much stronger than previously expected and it can be harnessed to repair and restore lost or compromised function of tissue and organ to the body.
2. Potentially Regenerative Cells (PRCs) in every tissue and organ of the body
To regenerate the lost tissue or organ, multiple cell types must be produced to form the new tissue. Where do these cells come from?
In a fully developed adult human body adult stem cells constantly participate in normal homeostatic production of functional mature cells to maintain the structural and functional integrity. Some in the field of stem cell research believe that adult stem cells reside in specific niches, such as epidermal stem cells in the bulge of a hair follicle, intestinal epithelial stem cells in the crypt at the base of the villus. Moore & Lemischka (2006) “Stem cells and their niches” Science 311:1880-1885. These stem cells, once destroyed, cannot be renewed.
Through two decades of clinical and basic research, Dr. Xu and the team of scientists and clinicians have found that in response to the injury and under the conditions provided by using MEBO technology and products, ordinary somatic cells residing at the site of the wound can be induced or activated to behave like stem cells—proliferate and differentiate orderly to provide multiple cell types to form new tissue with physiologically correct structure and function. For example, in a full-thickness burn wound the so-called “epidermal stem cell niches” in the bulge of hair follicle have been destroyed. However, under the condition provided by MEBO, viable cells at the wound site are converted into epidermal stem cells so as to provide multiple cell types to form new dermis and epidermis with the correct architecture, as well as appendages, nervous and vascular networks of the skin with normal physiological function. In addition, cultured under the condition provided by MEBO wound ointment, bone marrow cells from holes drilled on the bone at the wound site can be induced to differentiate orderly to produce multiple cell types that form new muscle, soft tissue and skin after burn injury that reaches the bone.
These results demonstrate that normal somatic cells in an adult body can be induced under specific conditions to behave like stem cells that proliferate and differentiate to produce various types of cells necessary to regenerate lost or damaged tissue.
What is the nature and dynamics of wound regeneration process under the conditions provided by MEBO?
3. The regeneration process recapitulates embryonic development process and mimics scar less wound regeneration of the fetus
By using tissue samples obtained from different time points during the regeneration process of the wounds in burn patients, Dr. Xu and his team obtained precious evidence showing dynamic changes of cells at both the cellular and tissue levels. By using immunohistochemical labeling of specific biomarkers, results were obtained that indicates that adult wound regeneration process under the conditions provided by using MEBT/MEBO recapitulates embryonic development and mimics scarless wound healing of the fetus.
Compared to fetal wound healing, the wound healing process in an adult with fully developed organs is carried out in a relatively more hostile environment than that for a fetus. The wound is susceptible to adverse effects caused by "normal" inflammatory response of the body to wounding and by exogenous agents such as bacteria that causes infection and further inflammation systemically and on the site. As discussed above, the prevailing thought in the art is that adult wound healing must be scarring healing because the adult-type, "normal" inflammatory wound healing is evolved to reduce the risk of infection at the expense of healing quality. The compelling results obtained in the clinical practice using MEBT/MEBO change this dogma by showing that an fully developed adult possesses an inherent ability of self-repair and regeneration in response to wounding if suitable conditions are provided exogenously, and the wound healing process can mimic that occurring in a fetus at the early gestation stage to result in scarless healing in severely damaged skin.
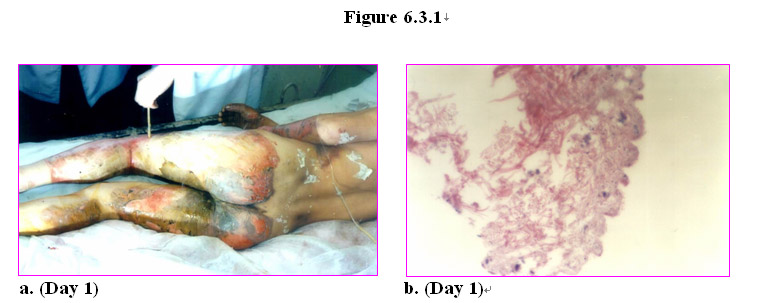
Figure 6.3.1 shows the representative changes in the cells and tissues in a full-thickness burn wound of a patient (Figure 6.3.1a) treated with MEBT/MEBO. Figure 6.3.1b shows that 24 hours post burn injury there was coagulation and necrosis of epidermis and degradation of collagenous fibrous in superficial layer of the dermis. In the presence of the MEBO wound ointment, the necrotic tissues in the superficial layer is liquefied and discharged gradually. Because the necrotic tissues are liquefied instead of being surgically removed, the remaining viable tissues are protected from secondary injury caused by surgery.
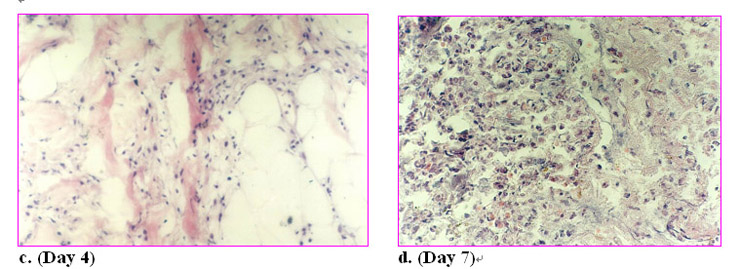
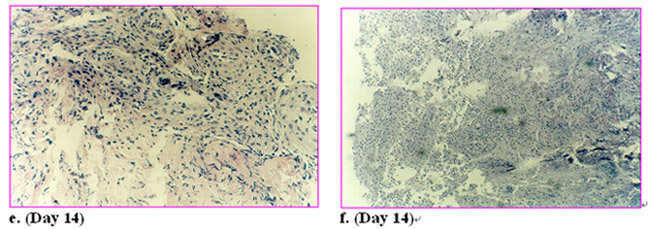
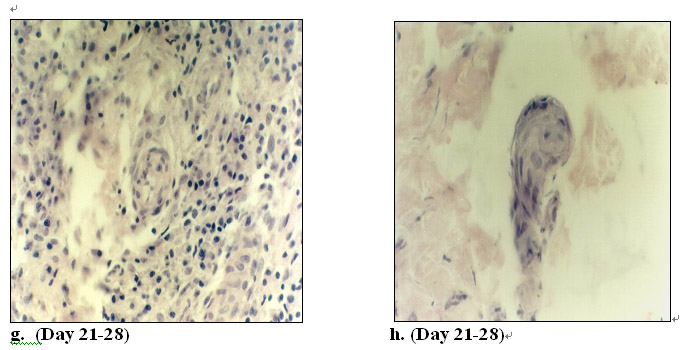
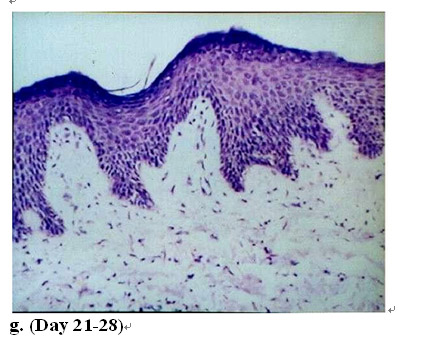
On day 4 post burn there was already high activity of regeneration at the wound site with active proliferation of cells in the interstitial subcutaneous tissue (Figure 6.3.1c). On day 7 post burn a large number of regenerative cells appeared at the wound site (Figure 6.3.1d). On day 14 post burn massive regenerative cells appeared and nascent tissue started to form at the wound site (Figure 6.3.1e&f). On day 21-28 post burn wound regeneration was near complete. The wound was covered by stratified squamous epithelium; blood vessels, nerve and most of the appendages such as hair folicles started to form in the dermis (Figure 6.3.1g&h). The skin was regenerated with normal structure as shown (Figure 6.3.1i). At a higher magnification under an electron microscope, the junction between the dermis and epidermis is completely natural. Moreover, collagenous fibers in the new skin are arranged in a normal order three-dimensionally. See Figure 1.2.2.9.
To monitor the dynamic changes of cells in growth and differentiation during the process of adult tissue and organ regeneration in vivo, wound regeneration of full-thickness burns is used as a clinical model to demonstrate how adult cells respond to exogenous agents under the treatment using MEBT/MEBO.
Dr. Xu and his research team demonstrated for the first time that embryonic epidermal stem cells are induced or activated and able to proliferate in adult human under conditions favorable for physiological tissue repair and organ regeneration. Such regenerative conditions are provided by using MEBT and by applying MEBO wound ointment topically to the wounds.
During the treatment of the patients with full-thickness burns, vigorous cellular activity on the wounds was observed in the presence of MEBO wound ointment. These “hyper-active” cells (Figure 6.3.1.c&d) are confirmed to be cells expressing keratin-19 detected by immunofluorescent staining with a monoclonal antibody against human keratin-19 (K-19).
The results summarized in Figure 6.3.2 show that in the normal adult epidermis, few cells were K-19 positive (Figure 6.3.2a). In contrast, for skin in the wounds, there was a moderate amount of regenerative epidermal stem cells that were stained positive for K-19 24 hr post burn (Figure 6.3.2b). On day 4 post burn (Figure 6.3.2c), the number of K-19 expressing cells increased around the sweat gland, capillaries and hair follicles. On days 7 and 14 epidermal stem cells continued to increase, reaching peak values during this period (Figure 6.3.2d and 6.3.2e, respectively). Until days 21 and 28, the number of K-19 expressing cells decreased to low levels (Figure 6.3.2f and 6.3.2g, respectively).
On day 30 post burn, electron microscopic examination of the sections taken from the new skin of the patient revealed that the skin regenerated by using the methodology of the present invention retains its normal, physiological structure. Also, the collagenous fibers in the regenerated new skin were normal in both size and spatial arrangement, measured 0.1-05 m and with characteristic light and dark periodic cross striation (64 nm). See Figure 1.2.2.9.
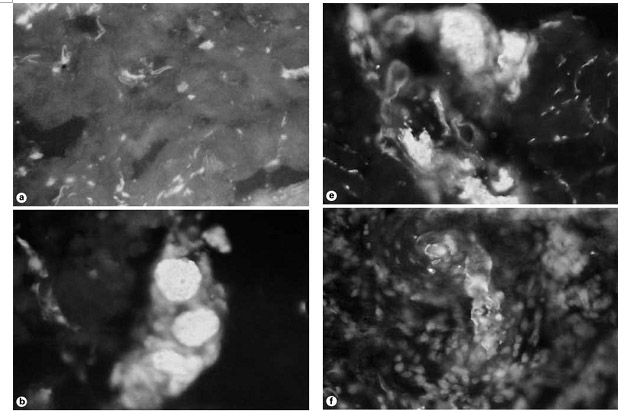
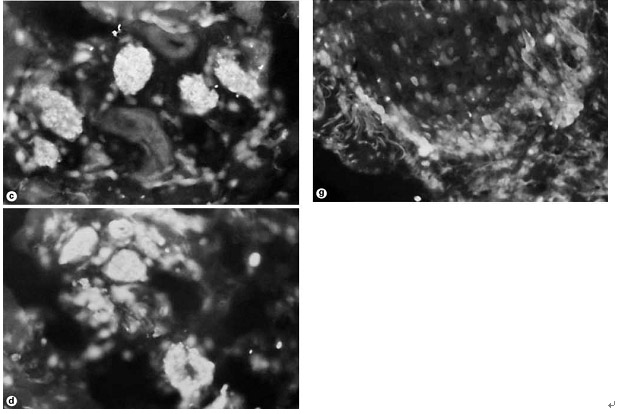
Figure 6.3.2. Stained frozen tissue sections using mouse anti-human keratin type 19 (K-19) monoclonal antibody (x200 magnification). a: Normal skin (No K-19 positive cells. b-g: After treatment with MEBO wound ointment. b: 24 h postburn (a few K-19 positive cells appeared). c: Day 4 postburn (the number of K-19 positive cells increased). d: Day 7 postburn (the number of K-19 positive cells peaked). e: Day 14 postburn (the number of K-19 positive cells plateaued). f: Day 21 postburn (the number of K-19 positive cells decreased). g: Day 28 postburn (the number of K-19 positive cells decreased significantly). See Xu (2004) in Burns Regenerative Medicine & Therapy, p.117, S. Karger AG, Basel, Switzerland.
Where do K-19 expressing cells come from?
In burn wounds of deep 2nd degree or higher, epidermal stem cells residing in the basal layer of epidermis are destroyed. More interestingly and challengingly, in burn wounds of full-thickness burn, the whole epidermis and dermis are destroyed with only the hypodermis, the fatty layer of the skin, remaining viable. Treatment of full-thickness burn wounds with conventional methods such as skin grafts or skin substitutes results in wound-closure with disfiguring scars and substantial loss of normal function of appendages of the skin and physiological networks of blood vessels and nerve.
However, as shown above, adult patients who sustained full-thickness burns, after treated with MEBT/MEBO, could recover with skin regenerated with substantial restoration of its structures and function. What is the source(s) of epidermal cells that compose to form the tissues that constitute the regenerated skin organ?
The results obtained in the treatment of burn patients reveal that at least part, if not all, of the epidermal cells are originated from embryonic epidermal stem cells expressing K-19.
Keratin-19 has been known to be a biochemical marker of skin stem cells emerged during the embryonic development. In normal adult human epidermis, there is no or few K-19-expressing keratinocytes present. Michel et al. (1996) “Keratin 19 as a biochemical marker of skin stem cells in vivo and in vitro: Keratin 19 expressing cells are differentially localized in function of anatomic sites, and their number varies with donor age and culture stage” J. Cell Science 109:1017-1028. Hsia et al. (2008) “Effects of topically applied acitretin in reconstructed human epidermis and the Rhino mouse” J. Investigative Dermatology 128:125-130.
As shown in Figure 6.3.2, the number of cells stained positive for K-19 increased dramatically while the body underwent active tissue repair and skin regeneration, and the number declined when the regeneration was complete. It is believed that these embryonic epidermal stem cells proliferated and differentiated to produce specific types of cells, including other types of keratinocytes expressing keratin 1, 9, 10, and 16 that moved upward towards the epidermis. The detection of high expression of the embryonic epidermal stem cell marker K-19 indicates that the regeneration of skin by using MEBT/MEBO may recapitulate embryonic development and mimic the scarless wound healing of the fetus.
Histological analysis of tissue samples taken from many patients reveals that the wounds treated with MEBT/MEBO manifest distinct characteristics of cellular proliferation, differentiation and migration that resemble those of early-gestation fetal wound healing. In the presence of MEBO, activation or induction of regenerative stem cells, including K-19 expressing epidermal stem cells, is followed by proliferation and directional differentiation of the stem cells into specific types of cells necessary for the regeneration of a fully functional skin including blood vessels, hair follicles, collagenous fiber, interstitium and nerves.
These experimental findings are groundbreaking and will have a profound impact on our understanding of the regenerative capacity of the human body. To our best knowledge, this is the first time embryonic epidermal stem cells are detected during the wound regeneration process in an adult human body. These stem cells are originated from adult somatic cells that are induced to behave like embryonic epidermal stem cells under the conditions provided by MEBO wound ointment and by using MEBT. Such induction occurs in situ and in vivo, i.e., at the wound site where the cells are cultured in a moist regenerative environment provided by the ointment. Neither stem cell transplantation nor genetic engineering is involved in this process.
In comparison, for a long time in the field of regenerative medicine a great deal of efforts has been focused on studying individual factors (wound healing factors and genes) contributing to regeneration. For example, many in the field are trying to grow and control proliferation and differentiation of embryonic stem cells ex vivo, hoping to replace defective/diseased cells/tissues with cell therapy (Murry & Keller (2008) “Differentiation of embryonic stem cells to clinically relevant populations: Lession from embryonic development” Cell 132:661-680), or to genetically manipulate adult somatic human cells to mimic embryonic stem cells, such as those induced pluripotent stem (iPS) cells (see review by Nishikawa (2008) “The promise of human induced pluripotent stem cells for research and therapy” Nat. Rev. Mol. Cell Biol. 9:725-729; and commentary by Cyranoski (2008) “5 Things to know before jumping on the iPs bandwagon” Nature 452:406-407).
Although human somatic cells can be rendered by exogeneous gene transfer to look more like stem cells, so far iPS cells differentiate chaotically to form teratomas in vitro. Although the adenovirus-transduced with transcription factors could convert mouse exocrine cells into insulin-producing beta cells, no functional pancreatic islet has formed by these genetically programmed cells. Zhao & Daley (2008) “From fibroblasts to iPS cells: induced pluripotency by defined factors” J. Cell Biochem. 105:949-955.
While these studies of embryonic stem cells and iPS cells enrich our knowledge about the biological functions and pliability of the human cells, currently practical applications of these cells to regeneration of the human body are still at various early stages of research and development.
By contrast, MEBO has demonstrated that by using a completely different approach—botanical-based products with superior proven safety profiles—to achieve regeneration of tissue and organ in situ and in vivo through induction of normal somatic cells residing at the site of tissue/organ damage to behave like stem cells. As shown above, the result is natural, physiological proliferation and differentiation of tissue following the body’s intrinsic genetic lineage, providing just enough multiple cell types to replace the lost or injured cells so as to restore its structural and functional integrity. Compared to the approach of ex vivo cultivation of human embryonic stem cells or iPS cells whose clinical efficacy and safety are yet to be determined, MEBO’s innovative approach with proven clinical success represents a more direct and safer way to help the body regenerate when needed.
4. Regenerative condition and environment
One of the critical steps of wound healing is to effective remove eschar or necrotic tissues so as to prevent or minimize infection. The most commonly used technique is surgical debridement which often leads to secondary surgical injury to the viable tissues which are critical for tissue repair and regeneration. On the other hand, enzymatic or chemical debridement may not be as effective and may exert cytotoxic effects on viable cells in general.
Owing to its unique oil-based formulation combining sesame oil extract and beeswax that provide a semi-solid structural framework at ambient temperature, MEBO wound ointment is found to be able to remove necrotic tissues through liquefaction and subsequent exudation out of the damaged site.
Figure 6.4.1.1 schematically illustrates the mechanism by which necrotic tissue is removed through liquefaction and subsequent discharge from the wound. When the ointment is applied to the wound and subsequently warmed up by the skin, the oil permeates the wound surface and breaks up the necrotic tissues into particles by surrounding them, thereby initiating a series of biochemical reactions including hydrolysis, enzyme digestion, randicity, saponification, lipidification, and esterification, which hydrolyze the large necrotic tissues into smaller tissues that are further digested enzymatically into small molecules. Such produced toxic, acidic substances are neutralized through randicity and saponification to produce non-toxic substances, which are then lipified and esterified reversibly to further reduce the toxicity of the acidic substances in the necrotic tissues, thereby minimizing further injury to the viable tissues at the wound site. At the same time the oil that has undergone such reactions loses its lipophilicity and, combined with the liquefied necrotic tissue, is discharged from the wound surface, while fresh oil from the dressing continues to permeate the wound surface, starting another round of such biochemical reactions.
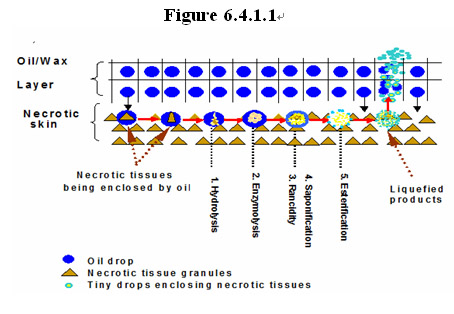
This noninvasive approach to wound debridment is advantageous in several aspects. First, the necrotic tissues are quickly removed and thereby are prevented from inducing inflammatory response of the body. Second, with the effective removal of the necrotic tissues, the conditions favorable for bacteria growth are destructed, thus dramatically reducing the risk of bacteria infection.
4.1 Unique mode of debridement via liquefication of necrotic tissues to minimize injury to viable tissues
One of the critical steps of wound healing is to effective remove eschar or necrotic tissues so as to prevent or minimize infection. The most commonly used technique is surgical debridement which often leads to secondary surgical injury to the viable tissues which are critical for tissue repair and regeneration. On the other hand, enzymatic or chemical debridement may not be as effective and may exert cytotoxic effects on viable cells in general.
Owing to its unique oil-based formulation combining sesame oil extract and beeswax that provide a semi-solid structural framework at ambient temperature, MEBO wound ointment is found to be able to remove necrotic tissues through liquefaction and subsequent exudation out of the damaged site.
Figure 6.4.1.1 schematically illustrates the mechanism by which necrotic tissue is removed through liquefaction and subsequent discharge from the wound. When the ointment is applied to the wound and subsequently warmed up by the skin, the oil permeates the wound surface and breaks up the necrotic tissues into particles by surrounding them, thereby initiating a series of biochemical reactions including hydrolysis, enzyme digestion, randicity, saponification, lipidification, and esterification, which hydrolyze the large necrotic tissues into smaller tissues that are further digested enzymatically into small molecules. Such produced toxic, acidic substances are neutralized through randicity and saponification to produce non-toxic substances, which are then lipified and esterified reversibly to further reduce the toxicity of the acidic substances in the necrotic tissues, thereby minimizing further injury to the viable tissues at the wound site. At the same time the oil that has undergone such reactions loses its lipophilicity and, combined with the liquefied necrotic tissue, is discharged from the wound surface, while fresh oil from the dressing continues to permeate the wound surface, starting another round of such biochemical reactions.
This noninvasive approach to wound debridment is advantageous in several aspects. First, the necrotic tissues are quickly removed and thereby are prevented from inducing inflammatory response of the body. Second, with the effective removal of the necrotic tissues, the conditions favorable for bacteria growth are destructed, thus dramatically reducing the risk of bacteria infection.
4.2 Formation of a respiratory membrane on the wound
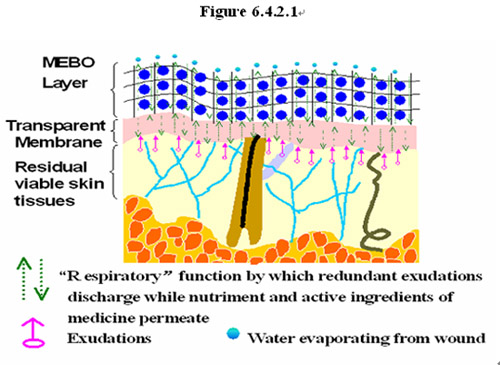
In the clinical studies of wound patients under the treatment using MEBT/MEBO, it has been found that after removal of necrotic tissues via liquefaction in the presence of the MEBO wound ointment the remaining viable tissues are not enclosed by the oil contained in the ointment; instead, they are protected by a layer of almost transparent membrane formed on their surface when the necrotic tissues are completely removed. As illustrated in Figure 6.4.2.1, a transparent proteinous membrane forms on the surface of the viable skin tissues, through which active ingredients in the ointment can permeate into the viable tissue to promote regeneration while the metabolic wastes and other exrecta can be discharged. This membrane acts as a protective layer isolating the fragile, nascent tissues that are undergoing active regeneration from the hostile environment outside. In a way, it serves as a substitute for the epidermis to protect the vital tissues in the dermis from environmental assaults. As illustrated in Figure 6.4.2.1, this membrane has a "respiratory" function which allows active discharging of metabolic waste and intake of nutrients and oxygen into the regenerating cells and tissues.
4.3 A unique mode of controlling and preventing bacterial infection without using conventional antibacterial agents
Clinical practice has revealed that MEBO can prevent wounds from infections. Xu (2004) Burns Regenerative Medicine and Therapy 1st ed., p. 77-82, Karger, Basel, Switzerland. In this clinical study, 14 burn patients were treated with MEBT/MEBO wound ointment, and bacteria isolated from the burn wounds were examined. It was found that Bacillus proteus had the morphological Hauch-ohne Hauch (H-O) variation, and the plasma coagulation ability of S. aureus decreased. In order to investigate the mechanism of the anti-infection effect of MEBO ointment, biological variability of Bacillus proteus, P. aeruginosa, E. coli, and S. aureus were cultured in medium containing various amounts of the ointment. The effect of the ointment on nonspecific immunity in vivo was also observed.
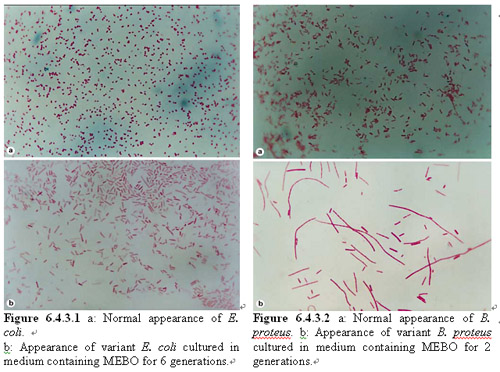
As shown in Figure 6.4.3.1, after proliferation to the 10th generation while cultured in MEBO ointment-containing medium, E. coli changed as follows: it lost motility, became sphere shaped, colonies became smaller, dry and flat. It was found that the decomposition activity of the bacteria to glucose and lactose was retarded after 32 hrs of culturing in the ointment-containing medium.
After being cultured for several generations on medium containing certain amounts of MEBO ointment, the motility of B. proteus gradually decreased before finally vanishing; and H-O transformation occurred. As shown in Figure 6.4.3.2, the 7th generation of the bacteria became long and filamentous. The decomposition activity of the bacteria to glucose and lactic acid was retarded.
Further in vitro bacterial culture experiments demonstrated that MEBO wound ointment possesses a unique ability to inhibit toxicity of a wide spectrum of bacteria commonly found on wounds. After continuous culture in medium containing MEBO ointment, many species of bacteria showed transformation in morphological structure and biological characteristics that are closely related with the growth environment. The morphological variation of bacteria may cause changes in its biochemical characteristics, antigenicity and toxicity.
In summary, the mechanism of the anti-infective effect of MEBO includes inducing transformation of the bacteria, decreasing their proliferation rate, reducing bacterial pathogenicity, and promoting nonspecific immunity of the body.
Compared with conventional methods of using antibiotics and alcoholic antiseptics, MEBO’s approach is directed toward a completely different mode of bacteria inhibition. MEBO demonstrated that the bacterial cells need not undergo fast and immediate cell death following application of the ointment. Instead, bacterial cells may still be capable of genetic replication but the toxicity of bacteria is severely inhibited by the ointment's interference with the bacterial cell division and thus the production of toxin. As shown in the above cell biological and microscopic studies, this inhibitory effect is likely achieved by modulating the morphology and cellular structures of bacterial cells and by changing the ecology of bacterial growth. This way, application of MEBO ointment locally to the wound could eliminate the need for the use of conventional local antiseptics such as alcohol that can be too harsh as to injure the nascent, fragile regenerative cells at the wound site.
4.4 Creating and sustaining physiological moist environment to promote regeneration
In preclinical studies and clinical practice, MEBO wound ointment has also been found to possess the ability to keep the wound in a physiological moist environment, which mimics the ideal environment for scarless wound repair and regeneration in the fetus. Under such favorable conditions, neither too dry (which would cause desiccation and threaten viability of the cells), nor too wet (which would cause maceration of the wound), the residual viable cells would be induced to behave like stem cells that proliferate and differentiate by following the natural genetic lineages in embryonic development to eventually regenerate the tissues needed to restore the structural and functional integrity of the body.
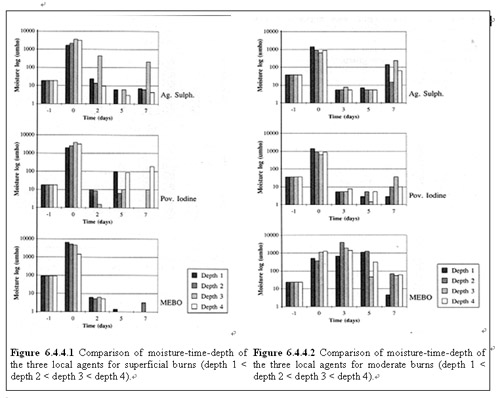
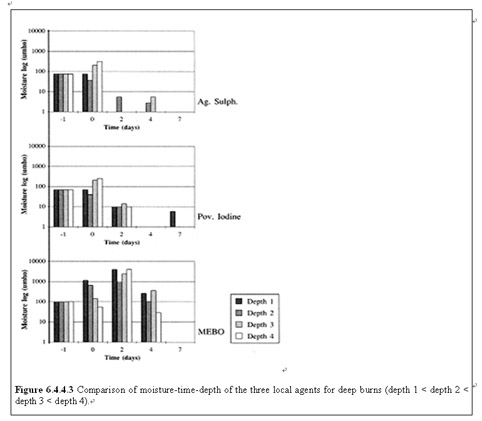
In the following animal studies, the ability of MEBO wound ointment to keep the wound in a physiological moist environment was evaluated on wounds of various depths in pigs, and compared with 2 commonly used topical agents for treating burn wounds: povidone iodine and silver sulphadiazine. Ioannovich et al. “Moist Exposed Burn Therapy: Evaluation of the Epithelial Repair Process (an Experimental Model)” Annal of Burns and Fire Disasters 2000: XIII (J):3-9.
As shown in Figures 6.4.4.1-3, based on the measurement of transepidermal water loss (TEWL) on the wounds of different depths (progressively from superficial to full-thickness burns), MEBO wound ointment consistently manifested a moisturizing environment for a longer period of time than other topical agents.
4.5 Clinical techniques for creating a regenerative local environment and condition
Over the past two decades of clinical practice using MEBT/MEBO, Dr. Xu and teams of clinicians in China Burns Association who have been trained by him have established and perfected clinical modalities for treating various types of wounds. Depending the extent, depth and systemic pathological condition of the patient, systemic and local treatment protocol may vary to some extent. However, in principle, critical steps involve the following.
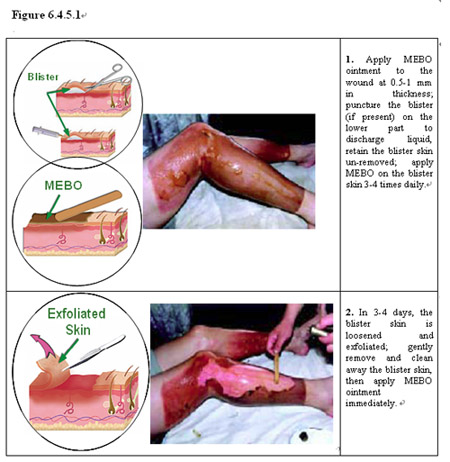
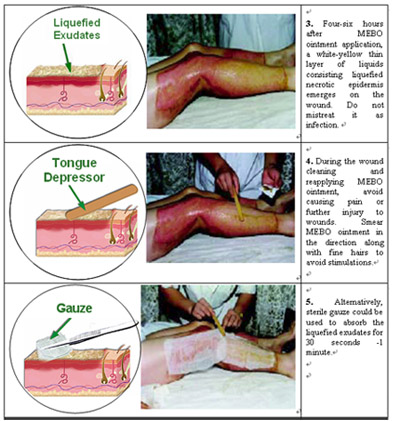
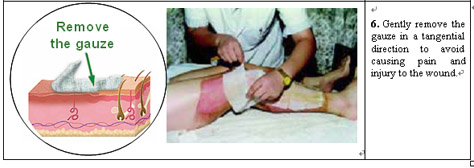
Generally the earlier applying MEBO wound ointment to the wound post injury, the better result. For the best result, applying the ointment within 4 hours after injury is desirable. The ointment should not be applied more than 1 mm in thickness to ensure underlying tissue’s proper ‘breathing’. Timely (4-6 hrs) cleaning of exudates, liquefied necrotic tissues, and ointment residues and re-applying the ointment is critical. Avoid causing pain, bleeding, or any secondary injuries to the wound when cleaning or making any necessary debridement. Do not make any aggressive surgical excisions. Keep wounds covered by the ointment all the time without desiccation and maceration. MEBO wound ointment should be applied throughout the treatment period with no interruption from other treatments. Water, desiccants, and any stimulative disinfectors should not be used for cleaning the wound site. If the wound is second degree or deeper, ‘translucent membrane’ may be formed on the wound surface during MEBO treatment. It should be protected when changing the dressing.
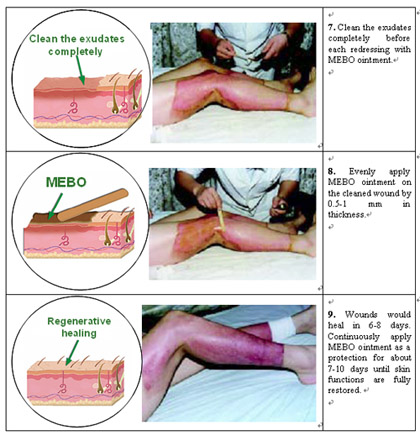
To illustrate these points, Figure 6.4.5.1 shows the typical steps taken in the clinical treatment of partial-thickness burns by using MEBT/MEBO.
stay informed. connect with us.